History:
A 13 y/o boy developed pain over his left elbow after a fall to the
ground.
Questions:
1. What are the findings?
2.What is the diagnosis?
Answers:
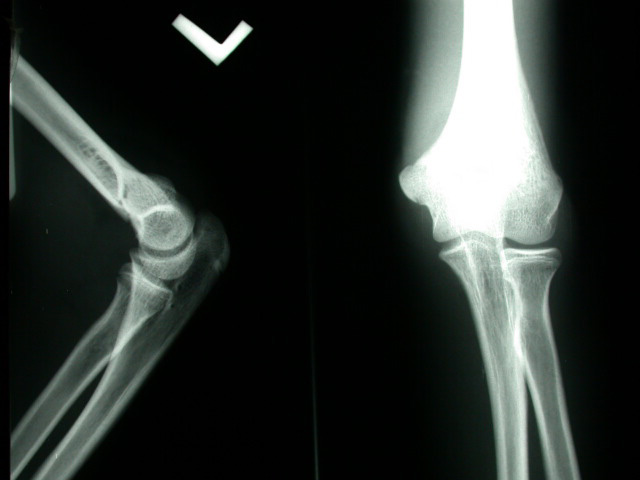
1. Anteroposterior (AP) and lateral radiography of the elbow:
l Prominent anterior and posterior fat-pad signs.
l Minimal displaced step off defect and a radiolucent line over
the distal humerus.
l There is slight posterior angulation of the distal humerus ..
2. Supracondylar fracture of the distal humerus
Discussion
The fat-pad sign at the elbow indicating an elbow effusion. Distension
of the elbow capsule by fluid lifts up the anterior and posterior
fat pads at the superior aspect of the elbow joint, displacing them
from their normal positions and rendering them visible radiographically
on the lateral view. A small portion of the anterior fat pad normally
is visible as a thin triangular radiolucency with a short base facing
the elbow joint; the posterior fat pad is contained fully within
the olecranon fossa and is not visible. In the setting of acute
trauma, the fat-pad sing is indicative of fracture, but an effusion
from any cause may result in a fat-pad sign. More than 90 % of children
or adolescents with posterior fat-pad sigh will have a demonstrable
fracture, and the absence of the fat-pad sign in this age groups
virtually excludes an intraarticular fracture, unless the injury
is so severe that there is disruption of the elbow joint capsule.
The supracondylar fracture comprises 60% of fractures around the
elbow in children. Radial head and neck fracture, common in adult,
generally are not seen in children. Supracondylar fractures occur
with hyperextension of the elbow, usually from a fall. The fracture
extends transversely across the distal humerus through the coronoid
and olecranon fossa, above the level of the condyles. The distal
fragment is angulated posteriorly, so that the anterior humeral
line passes anterior to the capitellum. A posterior fat-pad sign
almost always is present. The fracture usually is complete, but
greenstick fracture, torus fractures, or plastic bowing are possible.
The typical treatment is closed reduction with casting.
Reference
1. S. P. Bohrer. The fat pad sign following elbow trauma: its usefulness
and reliability in suspecting "invisible" fracture. Clin
Radiol 1970; 21: 90-94
|