|
History :
The 4+M/O girl was a case of diastematomyelia noted since birth
without ans dysfunction noted at present. This time, she was admitted
due to rapid enlargement of paraspinal mass in recent 5 days.
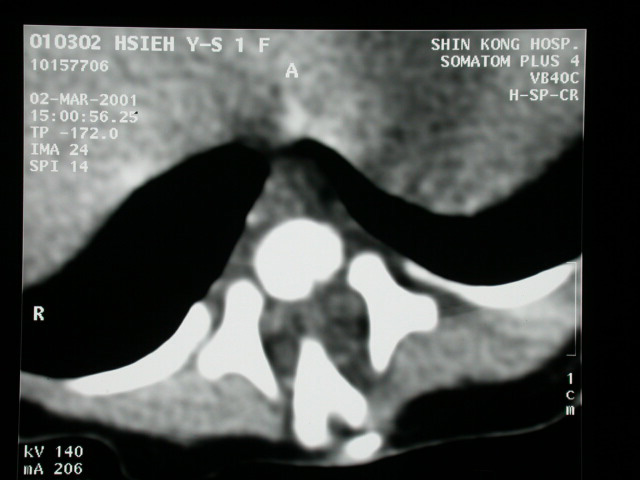
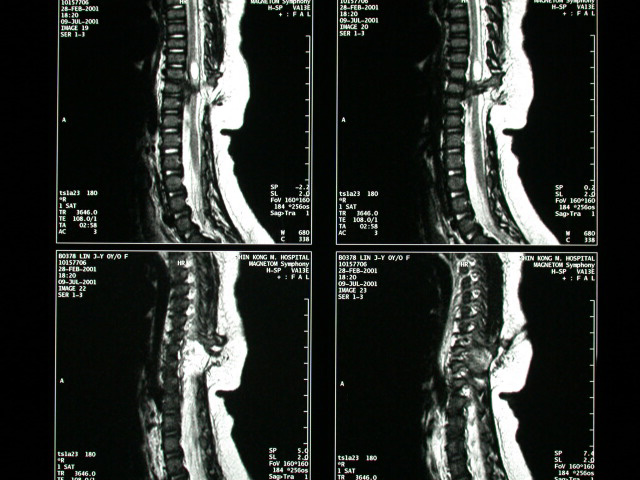
Image finding :
MRI of T-spine without & with contrast shows:
-Diastematomyelia with bony bridge and two hemicord are noted at
T9-T10.
-presence of syrinx above the lesion
-No definite abscess is detected.
Diagnosis :
Spina Bifida with overlying hemangioma. Diastematomyelia.
DIASTEMATOMYELIA
=SPLIT CORD
=sagittal division of spinal cord into two hemicords, each of which
contains a central canal, one dorsal horn + one ventral horn
Etiology:
congenital malformation as a result of split notochord; M:F = 1:3
Path:
--(a)2 hemicords each covered by layer of pia within single subarachnoid
space + dural sac (60%); not accompanied by bony spur / fibrous
band
--(b)2 hemicords each with its own pial, subarachnoidal + dural
sheath (40%); accompanied by fibrous band (in 25%), cartilaginous
/ bony spurs (in
Associated with:myelomeningocele
-hypertrichosis, nevus, lipoma, dimple, hemangioma overlying the
spine (26-81%)
-clubfoot (50%)
-muscle wasting, ankle weakness in one leg
Location: lower thoracic / upper lumbar > upper thoracic >
cervical
-congenital scoliosis (50-75%) 5% of patients with congenital scoliosis
have
-spina bifida over multiple
-anteroposterior narrowing of vertebral bodies widening of interpediculate
distance
-narrowed disk space with hemivertebra, butterfly vertebra, block
vertebra
-fusion + thickening of adjacent laminae (90%)
--(a)fusion to ipsilateral lamina at adjacent levels
--(b)diagonal fusion to contralateral adjacent lamina = intersegmental
laminar fusion
-bony spur through center of spinal canal arising from posterior
aspect of centra (<50%)
-thickened filum terminale >2 mm (>50%)
-tethered cord (>50%)
-low conus medullaris below L2 level (>75%)
-the 2 hemicords usually reunite caudal to cleft
-defect in thecal sac on myelogram
Cx
:progressive spinal cord dysfunction |