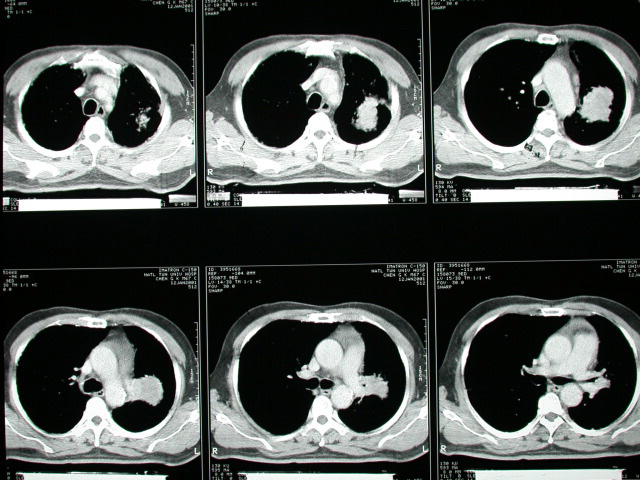
History :
This 68-year-old gentalman suffered from cough without sputum for
4 years.
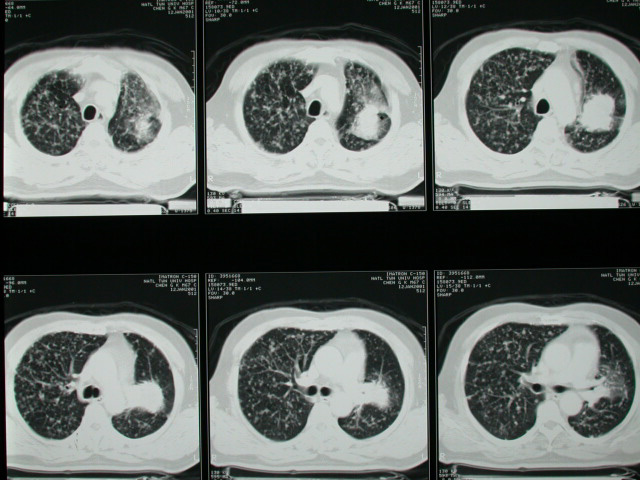
Image finding :
Numerous nodules in both lungs which compatible with hematogeneous
metastasis.
Diagnosis :
Lung Ca ( adenocarcinoma,stage IV) with hematogeneous carcinomatosis
Discussion :
Adenocarcinoma (50%)
Most common cell type seen in women + nonsmokers!
Location:
almost invariably develops in periphery; frequently found in scars
(tuberculosis, infarction, scleroderma, bronchiectasis) + in close
relation to preexisting bullae
-solitary peripheral subpleural mass (52%) / alveolar infiltrate
/ multiple nodules
-may invade pleura + grow circumferentially around lung mimicking
malignant mesothelioma
-upper lobe distribution (69%)
-air broncho- / bronchiologram on HRCT (65%)
-calcification in periphery of mass (1%)
-smooth margin / spiculated margin due to desmoplastic reaction
with retraction of pleura
PRESENTATION :
-solitary peripheral mass with corona radiata / pleural tail sign
/ satellite lesion
-cavitation (16%): usually thick-walled with irregular inner surface;
in 4/5 secondary to squamous cell carcinoma, followed by bronchioloalveolar
carcinoma
-central mass (38%): common in small cell carcinoma
-unilateral hilar enlargement (secondary to primary tumor / enlarged
lymph nodes) Nodes on CT:0-10 mm negative, 10-20 mm indeterminate,
>20 mm positive
-anterior + middle mediastinal widening (suggests small cell carcinoma)
-segmental / lobar / lung atelectasis (37%) secondary to airway
obstruction (particularly in squamous cell carcinoma)
-"S sign of Golden" = incomplete lobar collapse with bulging
contour produced by primary central tumor
-rat tail termination of bronchus
-bronchial cuff sign = focal / circumferential thickening of bronchial
wall imaged end-on (early sign)
-local hyperaeration (due to check-valve type endobronchial obstruction,
best on expiratory view)
-mucoid impaction of segmental / lobar bronchus (due to endobronchial
obstruction)
-persistent peripheral infiltrate (30%) = postobstructive pneumonitis
-NO air bronchogram
-pleural effusion (8-15%)
-bone erosion of ribs / spine (9%)
-involvement of main pulmonary artery (18%); lobar + segmental arteries
(53%) may result in additional peripheral radiopacity (due to lung
infarct)
-calcification in 7% on CT (histologically in 14%) usually eccentric
/ finely stippled
--(a)preexisting focus of calcium engulfed by tumor
--(b)dystrophic calcium within tumor necrosis
--(c)calcium deposit from secretory function of carcinoma (eg, mucinous
adenocarcinoma) |